UPlusE– A nationwide screening and early treatment project-
Depression in pregnancy and after childbirth
Perinatal depression affects 10–15% of mothers and approximately 5-10% of fathers. It is the most common complication in the first year postpartum. Early treatment is crucial, yet there is a notable underdiagnoses and undertreatment. According to insurance data provided by our partner BKK (Health Insurance) only 15% of those affected receive adequate treatment. If left unrecognized and untreated, it can have severe negative long-term consequences for the family’s health, leading to subsequent high costs.
What makes detection of peripartum depression so difficult?
Several factors are contributing to the low detection and treatment rates. Depressive symptoms are very similar to known circumstances of young parenthood (sleep disturbances, lack of energy, less activities). Symptoms like ambivalent or even lacking feelings towards the child are misinterpreted as personal deficiency (“being a bad mother/father”) and not as part of a treatable disease. The accompanying anxiety and shame are also the reason why patients do not actively seek help and try to preserve the image as “functioning mother/father” as long as possible. Even when symptoms are correctly assigned to a depressive disorder, the fear of stigmatization can delay the begin of treatment for a long time. A chance lies in the fact that questionnaires are answered more honestly than questions in the face to face situation during the doctor’s consultation.
What are the risks of peripartum depression?
These illnesses often become chronic, resulting in impairments in sensitive caregiving for the child, attachment disorders, child regulatory problems and in the worst case emotional neglect and abuse. Furthermore, suicide is one of the leading causes of death among mothers in the first year after childbirth. Early treatment of depression reduces individual suffering, enhances parenting skills and reduces healthcare system costs.
How to improve detection of peripartum depression?
Affected individuals are often seen during this time in gynaecological / paediatric practices but not by specialists in mental health. Consequently,
UPlusE aims to increase by implementing a screening for depression and psychosocial stress in perinatal and postpartum parents within routine obstetric and paediatric care with subsequent advice and—if necessary—further referral to a mental health specialist.
The UPlusE Screening
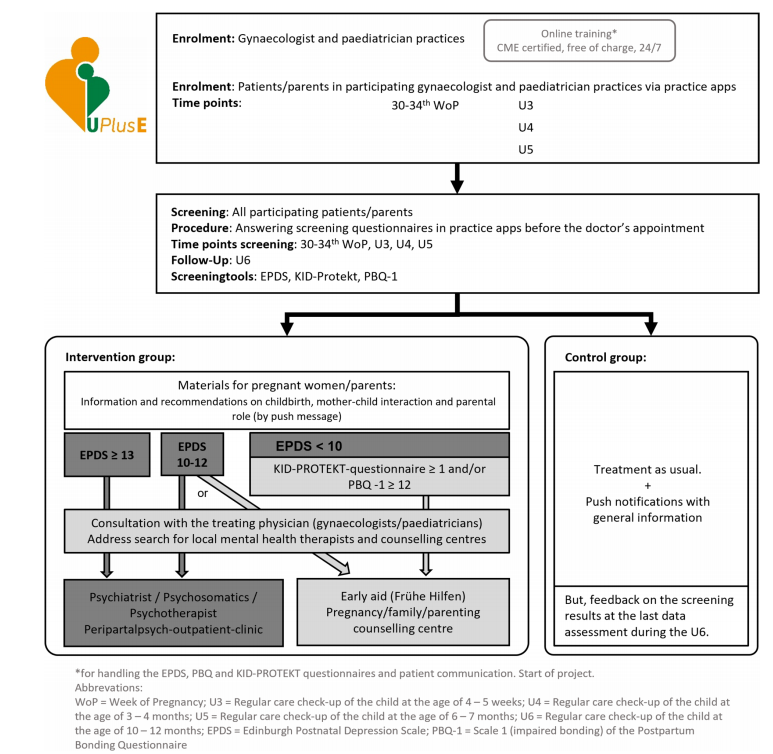
The new UPlusE Intervention starts with the first screening during the third trimester of pregnancy at the gynaecological check-up. Further screenings will take place after birth during paediatric check-ups U3-U6 (babies aged 1 month until 12 month).
The study participants will receive in preparation for each check-up the questionnaires upfront. During the following doctor’s appointment, the results will shortly be discussed. Depending on the individual results the physician will motivate the patient to turn to appropriate help (Forwarding scheme in attached graphic at the end of the document).
The UPlusE Questionnaires
Social-demographic questionnaire, pre-existing psychiatric conditions (only 1st screening)
Edinburgh postnatal depression scale (EPDS). Interpretation: 0-9 = no indication for depression, 10-12 = moderate, 13 points or more = high indication for depression.
KID-PROTEKT (psychosocial burdens)
Postpartum Bonding questionnaire (PBQ, scale “delayed bonding”, only in paediatric check-ups)
Schreien, Füttern, Schlafen (SFS, infant regulatory disorders)
Questionnaire on treatment/counselling utilization
Easy implementation of the UPlusE screening through Smartphone Apps
UPlusE uses established Apps (“Meine GynPraxis”/ “Meine pädiatrische Praxis”) throughout the entire screening and referral process. These apps are widely used for communication between patients and practices.
Automatic processes undertaken through the Apps:
- Presentation of the study information
- Sign-up process
- Presentation of the questionnaires and completion
- Immediate presentation of the results
- Links to more information and recommended referral
- Local search for counselling/therapy with contact information
- For the participating physicians: information about screening results and recommended referral + automatic medical practice billing
This makes the participation as easy as possible for the parents as well as the gynaecological / paediatric practices.
UPlusE – Network: early referral to mental health specialists
Not only early detection but also early treatment is essential. Therefore, a nationwide network of mental health specialists was established and is still growing. Until now more than 300 psychiatric and psychotherapeutic practices are part of the network. Participants with moderate or high indication for depression can turn to these addresses in order to receive an appointment as soon as possible (preferably within 2-4 weeks). Furthermore, UPlusE is cooperating with Kirinus, an online psychotherapy provider, with 200 additional therapists available.
UPlusE – online training for participating physicians
Participating physicians and mental health specialists receive a certified Continuing Medical Education (CME) online training free of charge, focusing on managing the screening
process and the management of peripartum mental health disorders.
UPlusE – Study and Forwarding Scheme
The UPlusE Screening takes place in participating practices since 02/2024 and until mid of 2026. During this time period 10.000 participants will be screened. The study is grant-aided by the Innovationsfonds (Federal Joint Committee). Participating gynaecologists and paediatricians receive compensation for the short discussion of screening results and referral.